
Runner's Knee: Causes, Treatment, and Prevention
What causes runner's knee and how do you fix it without stopping running? Learn the symptoms, real causes, at-home treatment, and the exercises that actually prevent flare-ups.
Published May 5, 2026 · Updated June 26, 2026

If your knee starts aching a few miles into a run — a dull throb right around the kneecap that gets worse going downhill or down the stairs afterward — there's a good chance you have runner's knee.
It is the single most common overuse injury in runners — patellofemoral pain is the most prevalent running-related injury, affecting an estimated 17–25% of runners every year. The good news: it is also one of the most fixable. Most cases resolve in 4–6 weeks with the right combination of rest, strengthening, and topical anti-inflammatory care — without surgery, without injections, and without giving up running for good.
This guide covers what runner's knee actually is, how to tell it apart from other knee injuries, what to do at home, and the four exercises that prevent it from coming back.
Contents
- What Is Runner's Knee?
- Symptoms: How to Recognize It
- The Real Causes (It's Not Your Knees)
- Runner's Knee vs IT Band vs Meniscus Tear
- At-Home Treatment That Actually Works
- 4 Exercises to Fix and Prevent Runner's Knee
- Returning to Running Safely
- When to See a Doctor
What Is Runner's Knee?
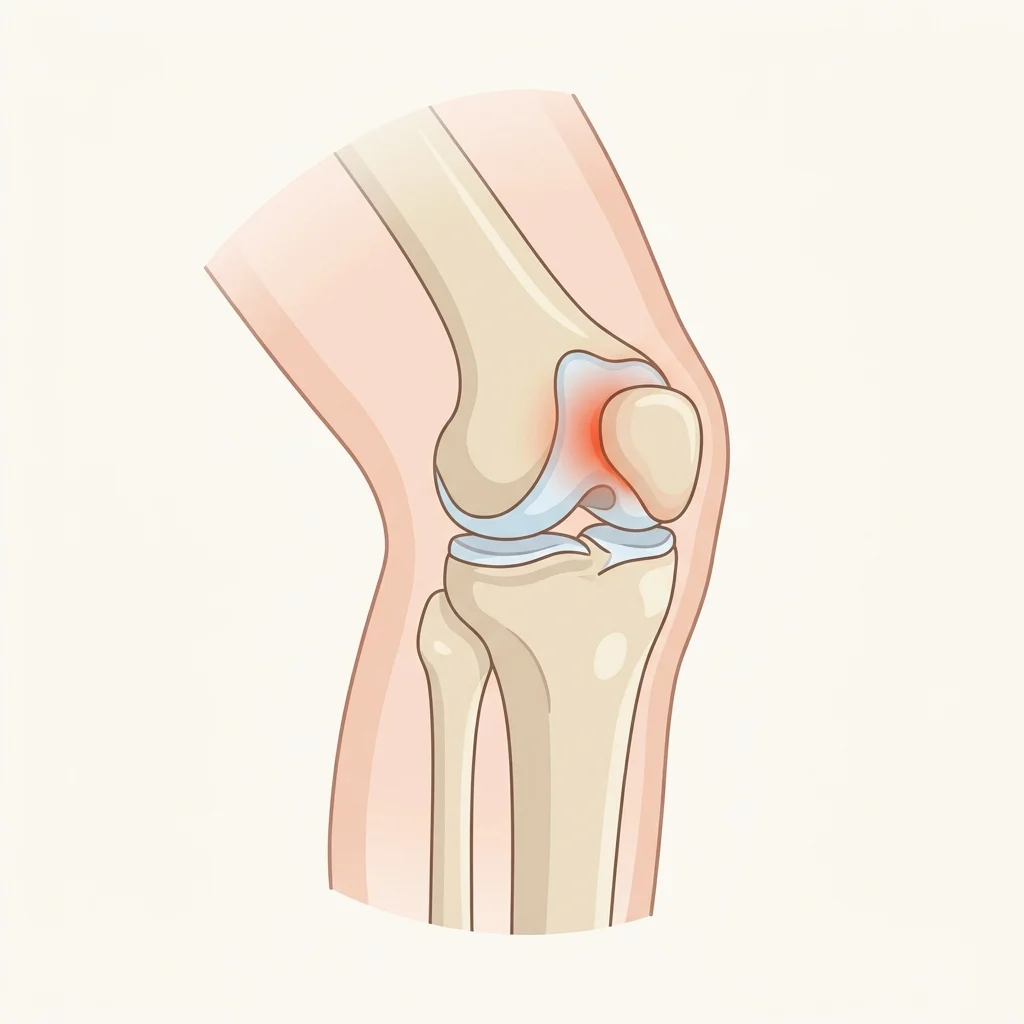
"Runner's knee" is the everyday name for patellofemoral pain syndrome (PFPS) — pain that comes from the joint between your kneecap (patella) and your thigh bone (femur).
Every time you bend your knee, the kneecap glides up and down a groove on the front of the thigh bone. When that motion is even slightly off-track — usually because the muscles that control it are weak or imbalanced — the cartilage on the underside of the kneecap gets compressed and irritated. Over thousands of footstrikes, that irritation becomes inflammation, and inflammation becomes pain.
It is not a tear, not arthritis, and not structural damage. It is a movement and load problem, which is exactly why fixing the movement (and managing the load) resolves it.
Symptoms: How to Recognize It
The classic runner's knee presentation is consistent across most people:
- Dull, aching pain around or behind the kneecap — not sharp, not stabbing
- Worse going downhill, down stairs, or squatting — anything that loads a bent knee
- Worse after sitting for long periods with the knee bent (the "theater sign" or "movie sign")
- Mild swelling or puffiness around the kneecap, not the joint itself
- Occasional grinding or clicking when bending the knee, usually painless
- Pain that builds during a run rather than appearing suddenly at one moment
If your pain showed up gradually, lives on the front of your knee, and behaves like the list above, runner's knee is the most likely diagnosis.
The Real Causes (It's Not Your Knees)
This is the part most runners get wrong. Runner's knee almost never starts at the knee. It starts above and below it.
1. Weak hips and glutes. The gluteus medius — the muscle on the side of your hip — controls how your thigh rotates with every step. If it's weak (and in most desk-bound adults, it is), your thigh rotates inward when you land, which drags the kneecap out of its groove. This is the single biggest driver of PFPS.
2. Quadriceps imbalance. The inner quad (vastus medialis) pulls the kneecap inward; the outer quad pulls it outward. When the outer is stronger — common in cyclists and runners who do a lot of mileage but no strength work — the kneecap tracks outward and grinds.
3. Sudden training spikes. Adding more than 10% weekly mileage, jumping into hill work, or signing up for a race and ramping fast all overload tissues that haven't adapted. Training errors like these are widely considered one of the leading causes of running injuries.
4. Worn-out shoes. Running shoes lose meaningful cushioning around 300–500 miles. Beyond that, every footstrike sends more shock up through the knee.
5. Hard or cambered surfaces. Concrete is considerably harder than asphalt, which is in turn far less forgiving than a dirt trail — and the harder the surface, the more shock travels up through the knee with every footstrike. Running every session on the same side of a cambered road also creates an asymmetric load.
6. Foot mechanics. Significant overpronation or very high arches change how force travels up the leg. This is real, but it's also overdiagnosed — most cases of runner's knee improve with strength work alone.
Runner's Knee vs IT Band vs Meniscus Tear
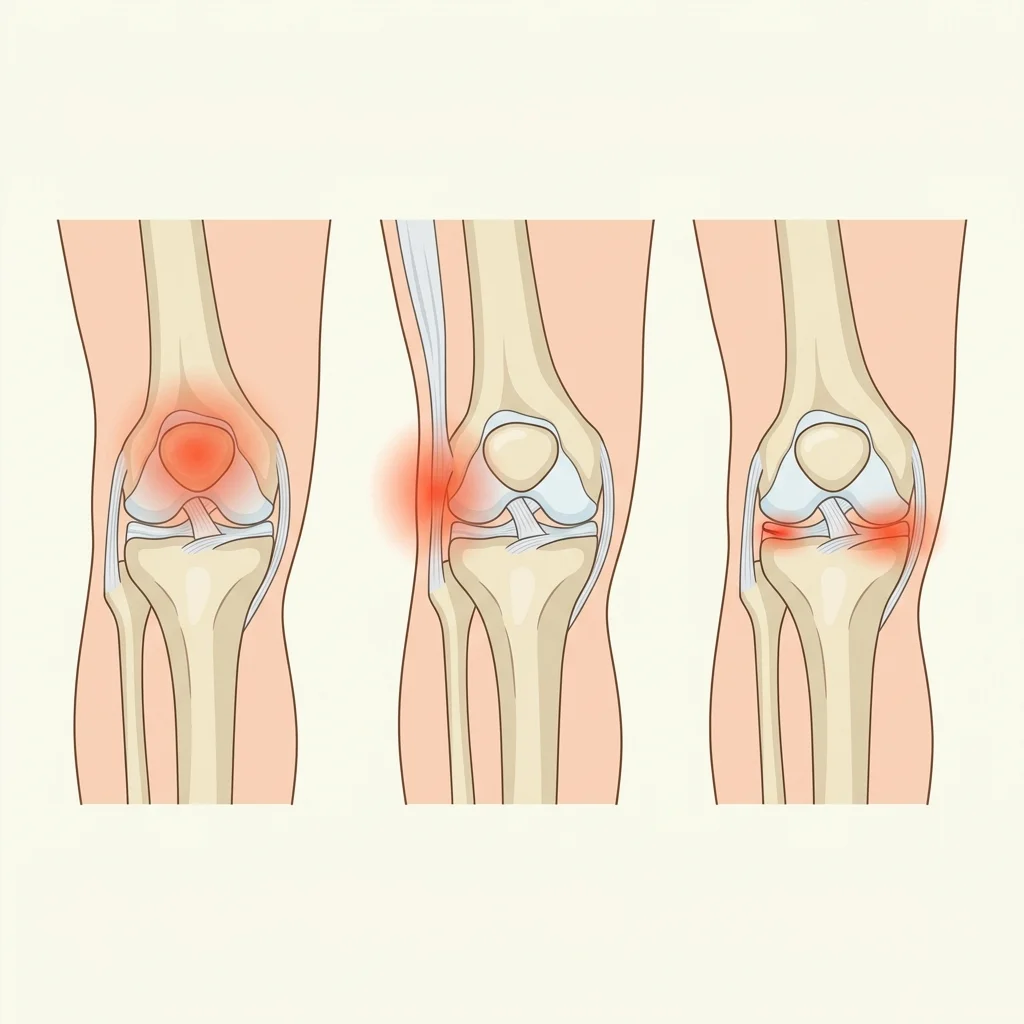
Three knee conditions get confused with each other constantly. The pain location and what triggers it usually tell them apart:
| Condition | Pain Location | Pain Type | Worst When |
|---|---|---|---|
| Runner's Knee (PFPS) | On or behind the kneecap | Dull, achy, builds gradually | Downhill, stairs, sitting bent |
| IT Band Syndrome | Outer side of knee | Sharp, burning, sudden | Specific mileage point, downhill |
| Meniscus Tear | Inner joint line, deep | Sharp, with clicking or locking | Twisting, deep squat |
| Patellar Tendinitis | Just below the kneecap | Tender to touch | Jumping, sprinting |
If your pain is sharp on the outer side and shows up at a predictable mileage point (often the same point every run), you're looking at IT band syndrome, not runner's knee. If it clicks, locks, or gives way — see a doctor and get imaging.
At-Home Treatment That Actually Works

For mild to moderate runner's knee, the at-home protocol below resolves the majority of cases inside a month.
1. Relative Rest, Not Total Rest
Stop running for 5–10 days, but keep moving. Cycling at a high seat (so your knee doesn't bend deeply), swimming, and pool running maintain fitness without loading the patellofemoral joint. Total bed rest actually slows recovery — cartilage gets nutrients from movement.
2. Manage Inflammation Locally
Oral NSAIDs (ibuprofen, naproxen) work but come with stomach, liver, and kidney costs if you take them for weeks — and runner's knee usually takes weeks. Topical herbal patches are a much better fit for this kind of multi-week, single-joint inflammation: they deliver active ingredients directly to the patellofemoral joint, give 8–12 hours of continuous relief, and bypass the digestive system entirely.
The Mrjoint Knee Relief Patches use a transdermal herbal formulation with capsaicin, wintergreen, camphor and safflower — the same anti-inflammatory and circulation-boosting ingredients used in traditional Chinese medicine for centuries — applied directly over the kneecap for 8–12 hours at a time.
For a deeper comparison of the two approaches, see Pain Patches vs Painkillers: Which Is Better for Joint Pain?.
3. Compression and Patellar Tracking
A compression knee brace does two jobs at once: it improves kneecap alignment so the patella tracks properly through its groove, and it provides proprioceptive feedback that helps you avoid the inward-knee collapse that caused the problem in the first place.
The Mrjoint Knee Brace provides patellar support and adjustable compression — useful in the first 2–4 weeks of recovery and during the early stages of returning to running. For a full breakdown of brace types and how to pick one, read our knee brace buying guide.
4. Ice After Activity, Heat Before
Apply ice for 15 minutes after any activity that aggravates the knee — this controls fresh inflammation. On rest days or before easy walking, use gentle heat to increase circulation to the area and loosen surrounding tissue.
4 Exercises to Fix and Prevent Runner's Knee

These four exercises target exactly the muscles that fail in PFPS. Do them 3–4 times a week. You should feel improvement within 2 weeks and be largely pain-free in 4–6.
1. Single-Leg Glute Bridge
Targets: Glutes, hamstrings, core stability How: Lie on your back, knees bent, feet flat. Lift one leg straight up. Drive through the heel of the planted foot to lift your hips until your body forms a straight line. Pause 2 seconds. Lower with control. Sets: 3 × 10 each leg
2. Side-Lying Hip Abduction (Clamshell)
Targets: Gluteus medius — the muscle whose weakness causes most runner's knee How: Lie on your side, knees bent at 90°, heels stacked. Keeping heels together and pelvis still, open the top knee like a clamshell. You should feel it deep in your side glute, not in your low back. Sets: 3 × 15 each side
3. Wall Sit with Ball Squeeze
Targets: Inner quadriceps (vastus medialis), the muscle that pulls the kneecap into proper alignment How: Sit against a wall with thighs parallel to the floor. Squeeze a small ball or rolled towel between your knees. Hold. Sets: 3 × 30–45 seconds
4. Step-Down
Targets: Quad strength and knee control under load — the exact pattern of running downhill How: Stand on a low step (4–6 inches). Slowly lower the opposite heel toward the floor, keeping the working knee tracked over the middle of your foot. Tap, don't bounce. Drive back up through the heel. Sets: 3 × 8–10 each leg
For more knee-specific strengthening work, see 10 Strengthening Exercises To Prevent Knee Pain.
Returning to Running Safely

Coming back too fast is how runner's knee becomes chronic. Use this conservative progression:
- Week 1: Walk-run intervals — 1 minute easy run, 2 minutes walk, repeated for 20 minutes, twice that week
- Week 2: 2 minutes run, 1 minute walk, for 25 minutes, three times that week
- Week 3: Continuous easy running, 20–25 minutes, three times that week
- Week 4: Return to roughly 60–70% of pre-injury weekly mileage
Three rules during the return:
- No pain above 2/10 during a run, ever. Sharp pain or pain that changes your stride means stop and walk home.
- No back-to-back run days for the first 3 weeks. Cartilage adapts slower than muscle.
- Run on softer surfaces — dirt trails, treadmills, or rubberized tracks — until you've had two pain-free weeks.
Pair the return with at least two strength sessions per week using the four exercises above. Strength is what makes the fix permanent.
When to See a Doctor
Most runner's knee resolves at home. See a sports medicine doctor or physical therapist if:
- Pain is severe or sharp, especially with twisting or pivoting
- The knee clicks, locks, or gives way under your weight
- You see significant swelling inside the joint (not just puffiness around the kneecap)
- Pain has not improved at all after 4 weeks of consistent treatment
- You felt or heard a pop at the moment pain started
These signs point to something more than PFPS — a meniscus tear, ligament injury, or cartilage damage — and need imaging to diagnose.
The Bottom Line
Runner's knee is a movement problem, not a knee problem. Fix the hips and quads, manage inflammation locally with topical patches and a compression brace instead of stacking weeks of oral NSAIDs, and rebuild your mileage gradually. Done consistently, this resolves the vast majority of cases inside 4–6 weeks — and prevents it from coming back.
If you're in the middle of a flare-up right now, the fastest path forward is the combination protocol: Mrjoint Knee Relief Patches for continuous targeted anti-inflammation, the Mrjoint Knee Brace during activity for tracking and compression, and the four exercises above 3–4 times a week.
Related Articles
- 10 Strengthening Exercises To Prevent Knee Pain – The full strength program for healthy and recovering knees.
- How to Choose the Right Knee Brace – Complete Buying Guide – Pick the right brace type for runner's knee, arthritis, or ACL recovery.
- 15 Natural Home Remedies For Knee Pain Relief – Non-pharmaceutical options for ongoing knee pain.
- Pain Patches vs Painkillers: Which Is Better for Joint Pain? – Why topical treatments fit multi-week injuries better than oral NSAIDs.

